Refractory Osteoarthritis: insights on the challenges
Evaluating the prevalence of Refractory Osteoarthritis
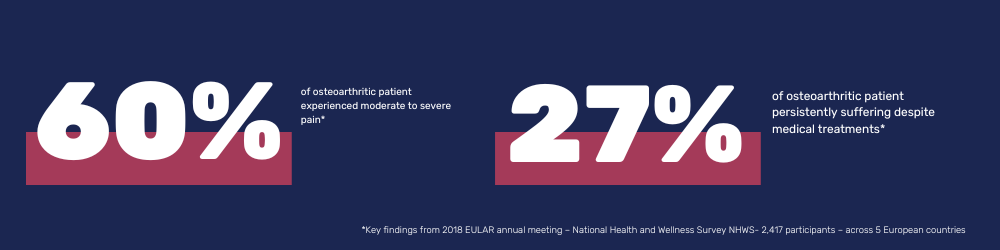
Osteoarthritis is a highly prevalent and debilitating joint disease that affects hundreds of millions of people worldwide, with almost 10% of the global population over the age of 60 being concerned1. The knee is the most commonly affected joint and knee osteoarthritis results in the destruction of the integrity of the cartilage and corresponding pathological changes in the joint edges and subchondral bones. Knee Osteoarthritis is a highly disabling condition with considerable impacts on patients’ daily lives.
While many subjects find relief through standard treatments, a substantive subset of patients are refractory to these therapies. Conventional treatments often employed—ranging from hyaluronic acid (HA) injections, corticosteroids, and pain-relief medications, to more invasive approaches like surgery—are unfortunately inadequate, leaving patients suffering from refractory Osteoarthritis in continued discomfort and seeking alternative solutions2.
What exactly is Refractory Osteoarthritis?
Osteoarthritis is a multifaceted condition, and its treatment can be complex. However, in certain instances, the standard treatments might not bring the anticipated relief. This gives rise to what’s termed as “refractory” osteoarthritis.
Refractory Osteoarthritis extends beyond the conventional definition of Osteoarthritis, characterized by a chronic failure to respond to standard modalities of treatment. The intricacy of refractory Osteoarthritis arises from a multitude of factors, including the heterogeneity in patient physiology, comorbid conditions, and the multifactorial nature of Osteoarthritis itself. Refractory osteoarthritis stands as the outlier in the continuum of this ailment, representing those cases that resist conventional therapeutic measures3.
Deeper understanding
The term “refractory” in the context of Osteoarthritis varies across rheumatology publications. Most commonly, it is used to describe situations wherein:
- Persistence of Osteoarthritis pain despite the use of conservative non-pharmacological treatments.
- Persistence of Osteoarthritis pain despite commonly used and recommended pharmacological treatments.
- Persistence of Osteoarthritis pain in advanced cases haven undergone well-conducted surgical treatment.
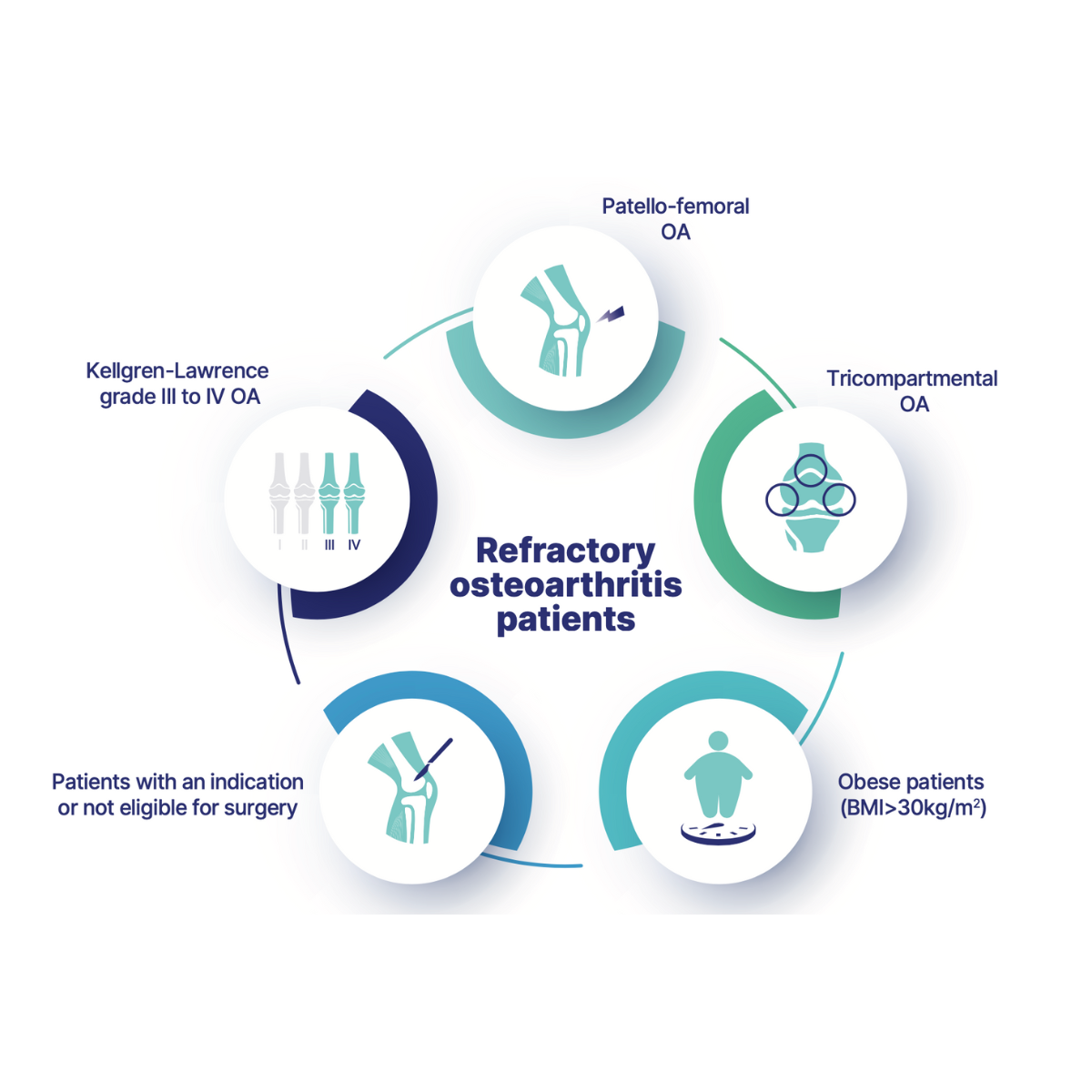
In the broader discussion about the effectiveness of knee osteoarthritis treatments, especially with hyaluronic acid (HA) viscosupplementation, certain patient phenotypes have been identified as potential predictors for non-responsiveness to HA-viscosupplementation.
The EUROVISCO group of experts notably identified some of these patient phenotypes in their 2018 publication4. These subjects, therefore, in addition to others identified in clinical practice, constitute a clearly-defined group of refractory Osteoarthritis patients.
Following on from the complexities of refractory osteoarthritis, one comes to a pivotal intervention –the TKR (total knee replacement). When knee osteoarthritic pain becomes unresponsive to all medical and physical treatments, TKR usually emerges as the final option for eligible patients.
However, the prevalence of TKR procedures brings with it an increasing strain on the healthcare systems. And, even more concerning, post- TKR surgery, which is often seen as the final therapeutic option, still leaves 10 to 20% of patients grappling with refractory knee pain. This poses significant challenges for both patients and healthcare systems.
Identifying the causes of Refractory Osteoarthritis
Determining the root causes of refractory Osteoarthritis is essential for more effective treatments. As research delves into the molecular mechanisms, new therapeutic strategies emerge.
Research spanning two independent patient cohorts experiencing refractory pain one year after total knee arthroplasty (TKA) revealed significant metabolomic associations, with one study concluding that patients with refractory osteoarthritis exhibited increased inflammatory and oxidative responses, which play a significant role in the clinical symptoms of refractory OA (the Newfoundland Osteoarthritis Study- NFOAS and the Longitudinal Evaluation in the Arthritis Program Osteoarthritis Study -LEAP OA 1 ).
Pathophysiology is central in differentiating refractory Osteoarthritis from its non-refractory counterpart. Refractory Osteoarthritis appears to have a heightened innate immune response, with elevated levels of inflammatory cytokines. These cytokines exacerbate cartilage degradation by promoting matrix metalloproteinases (MMPs) and aggrecanases, enzymes that destroy cartilage matrix5. Moreover, increased oxidative stress has been reported in these patients, highlighting a potentially vicious circle: inflammation incites oxidative stress, which in turn amplifies inflammation6.
The pathophysiology is believed to involve persistent low-grade inflammation, leading to a cycle of cartilage degradation, altered subchondral bone remodeling, and synovial inflammation, which standard interventions fail to adequately address. This relentless cycle not only contributes to the progression of joint damage but also to the chronic pain and disability often seen in these patients.
This knowledge highlights the limitations of current treatment modalities. If conventional treatments fall short, what’s the next step in our therapeutic journey for these patients?
